Catecholamine-producing neuroendocrine tumors of chromaffin cells of the adrenal medulla (85%) or of a paraganglion (paragangliomas, PGLs).
10% tumour:
10% inherited
10% extra-adrenal
10% malignant
10% bilateral
10% occur in children
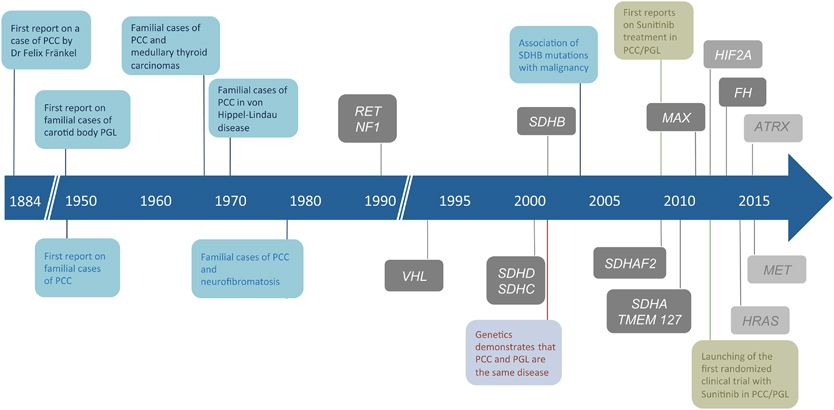
History:
Castro-Vega, L. J., Lepoutre-Lussey, C., Gimenez-Roqueplo, A.-P., & Favier, J. (2016). Rethinking pheochromocytomas and paragangliomas from a genomic perspective. Oncogene, 35(9), 1080–1089. https://doi.org/10.1038/onc.2015.172
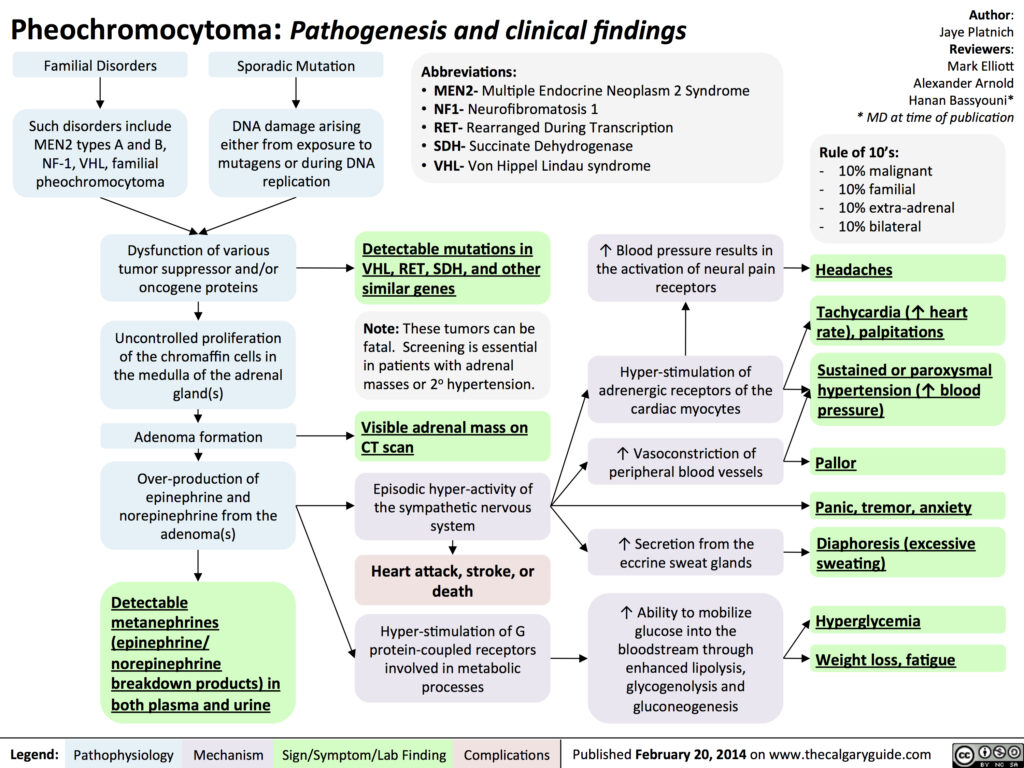
Etiology
This tumor secretes excessive amounts of catecholamines, leading to a variety of symptoms including hypertension, a pounding headache and tachycardia. Pheochromocytoma has a similar presentation to a paraganglioma, which originates from sympathetic nervous tissue as opposed to pheochromocytoma. However, both pheochromocytoma and paragangliomas are managed and treated similarly, so often are categorized together.
Tumour syndromes:
Hereditary pheochromocytomas occur with tumour syndromes
Multiple endocrine neoplasia type 2 (MEN 2)
Familial paraganglioma (PG) syndrome
von Hippel-Lindau (VHL) syndrome
Neurofibromatosis (NF) type 1
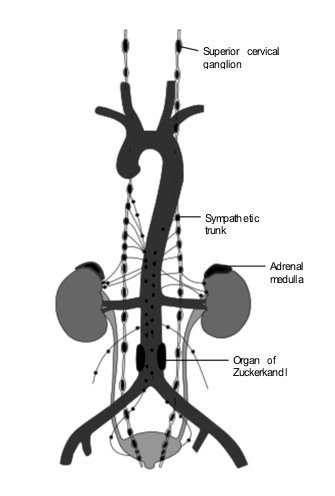
Extra-adrenal pheochromocytomas sites:
Abdomen (below diaphragm)
M/C site: Organ of Zuckerkandl: Chromaffin body derived from neural crest located at the bifurcation of the aorta or at the origin of the inferior mesenteric artery
Anatomic distribution of chromaffin tissue. | Lack E: Tumors of the adrenal gland and extra-adrenal paraganglia. In Armed Forces Institute of Pathology: Atlas of Tumor Pathology. Washington, DC, Armed Forces Institute of Pathology, 1997, 261–267
Presentation
Known as the great masquerader because of its variable clinical presentation. Presents with intermittent symptoms due to catecholamine excess.
Clinical triad:
Present in 90% cases
Headache (M/C symptom)
Profuse sweating
Palpitation & tachycardia
Other features:
Hypertension (90% cases) (M/C sign): Paroxysmal (50-60%) or continuous (30%)
Pallor (40-45% cases)
Weight loss (20-40% cases)
Hyperglycemia (40% cases)
Nausea (20-40% cases)
Anxiety & panic attacks (20-40% cases)
Orthostatic hypotension
Hypercalcemia
Polyuria and polydipsia
The Calgary Guide | http://calgaryguide.ucalgary.ca/
Utility of PPGL catecholamine phenotypes, as reflected by patterns of increases in plasma normetanephrine (NMN), metanephrine (MN), and methoxytyramine (MTY), for predicting tumor location, underlying mutation, and malignant risk. | Eisenhofer, G., & Peitzsch, M. (2014). Laboratory Evaluation of Pheochromocytoma and Paraganglioma. Clinical Chemistry, 60(12), 1486 LP-1499. https://doi.org/10.1373/clinchem.2014.224832
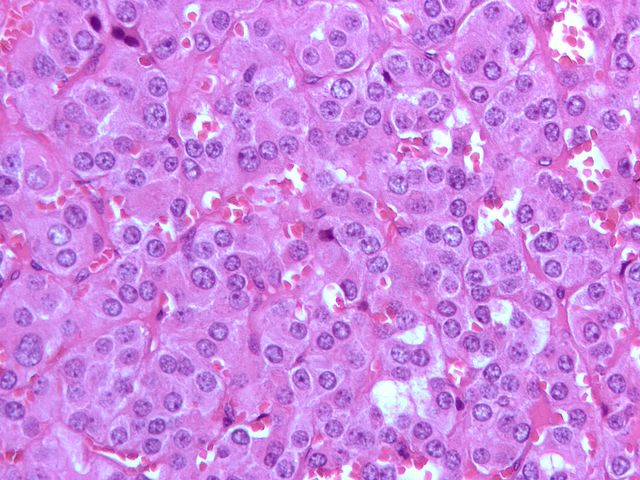
Tissue biopsy:
No FNAC since PCC is a vascular tumour
Micrograph of a pheochromocytoma (at high magnification) showing the characteristic arrangement of cells (Zellballen) and stippled (finely granular) chromatin. The chromatin pattern is sometimes referred to as “salt-and-pepper” chromatin. | By Nephron – Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=5938524
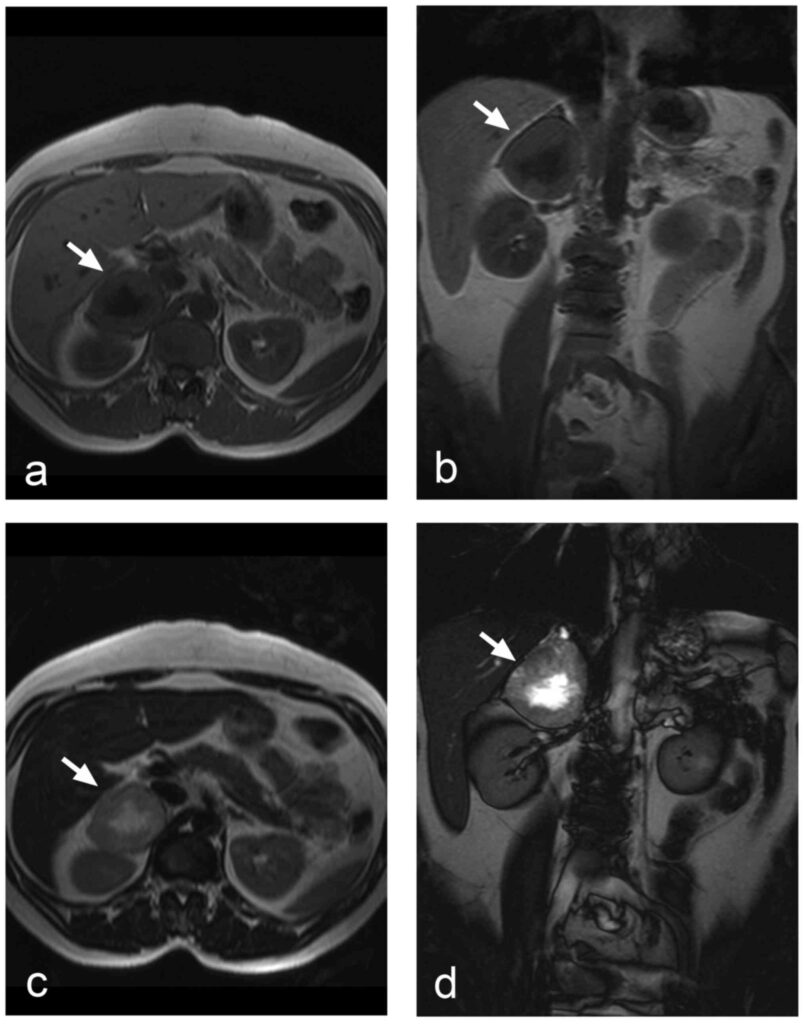
MRI:
Investigation of choice for localization (more specific/sensitive)
Adrenal pheochromocytoma on the right side (arrows): (a) T1-weighted spoiled gradient echo in the axial plane, (b) T1-weighted spoiled gradient echo in the coronal plane, (c) T2-weighted turbo spin echo in the axial plane, (d) True FISP in the coronal plane. T2-weighted image showing typical high signal intensity in the central necrotic part, which appears hypointense in T1-weighted images. | Eisenhofer, G., & Peitzsch, M. (2014). Laboratory Evaluation of Pheochromocytoma and Paraganglioma. Clinical Chemistry, 60(12), 1486 LP-1499. https://doi.org/10.1373/clinchem.2014.224832
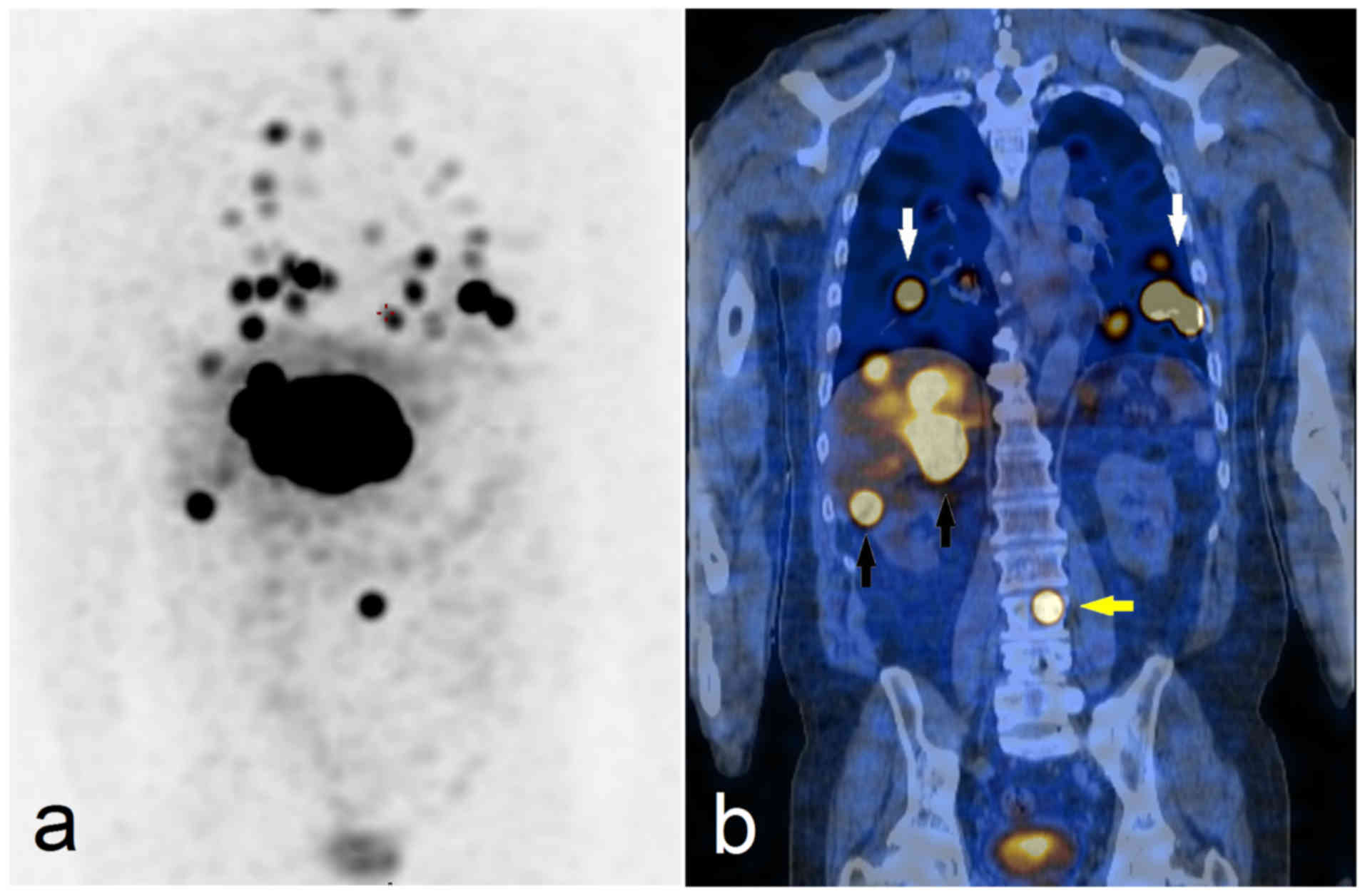
Nuclear scanning:
Fluorodopa-PET CT (GOLD STANDARD for localization)
123I-metaiodobenzylguanidine (mIBG) scintigraphy
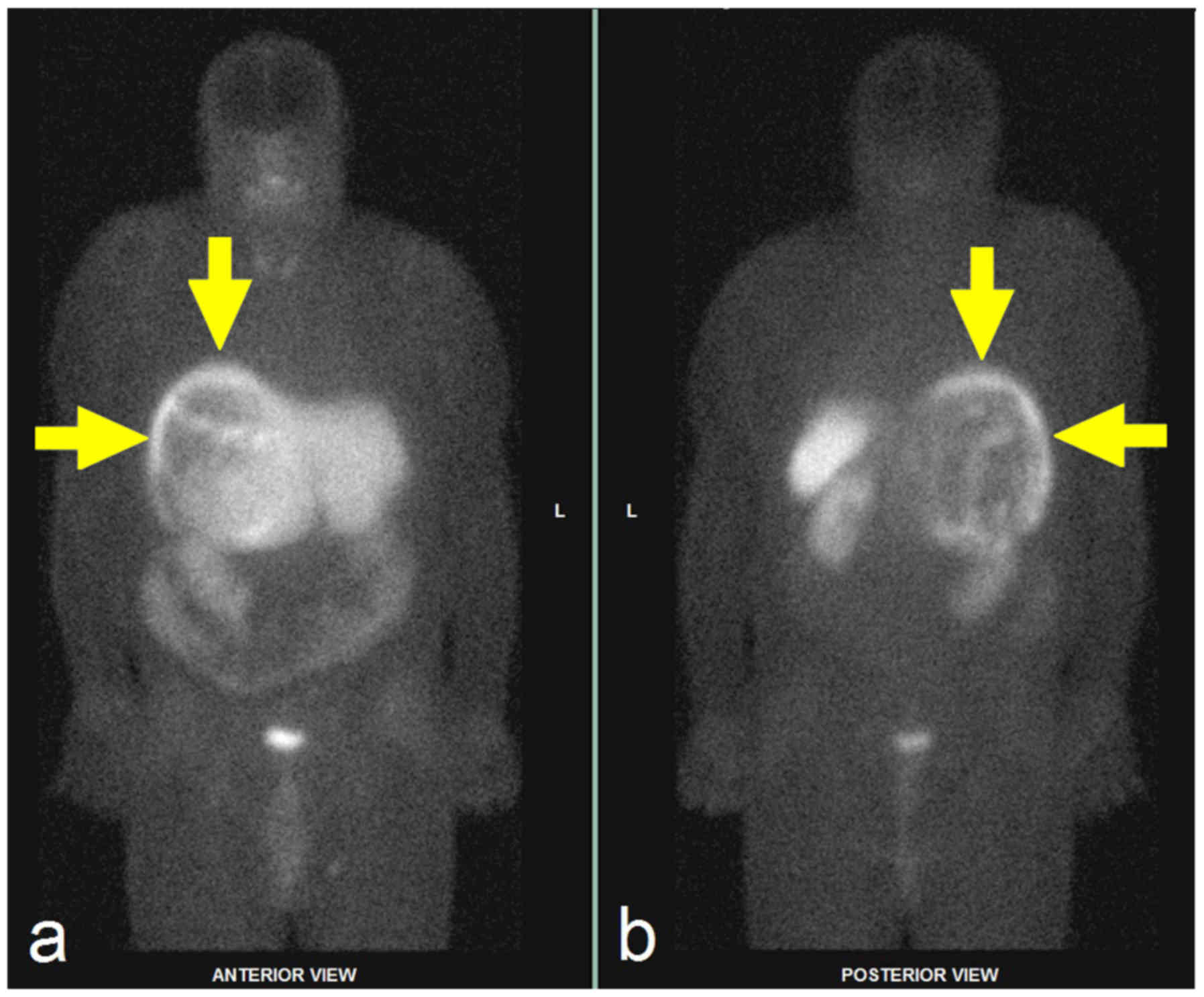
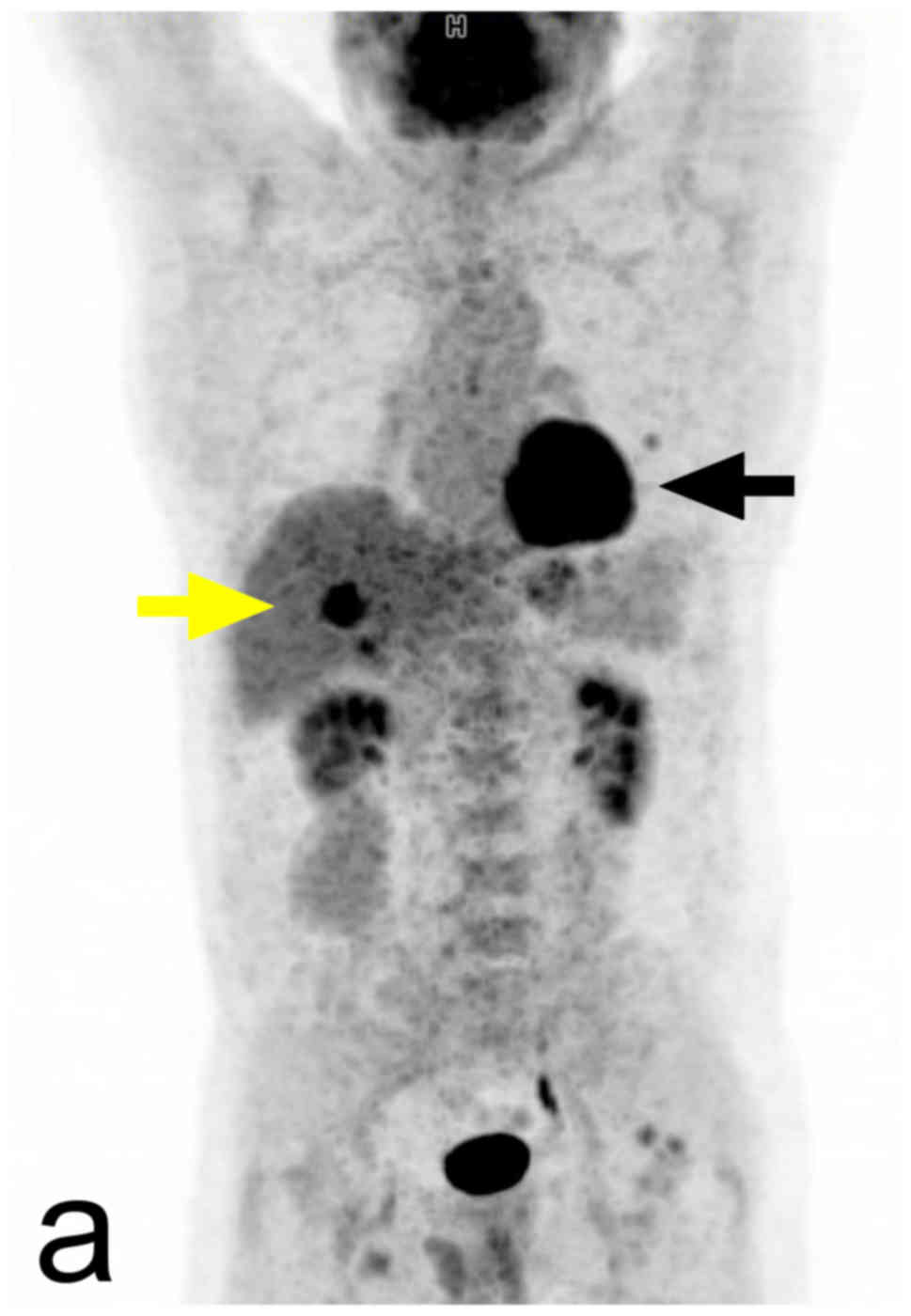
123I-MIBG SPECT/CT study: (a) maximum-intensity projection, (b) coronal slice. Re-staging examination reveals the metastatic spread of malignant pheochromocytoma into the lungs (white arrows), liver (black arrows), and vertebra L3 (yellow arrow). The patient subsequently underwent 131I-MIBG therapy. I-MIBG, I-metaiodobenzylguanidine. | Eisenhofer, G., & Peitzsch, M. (2014). Laboratory Evaluation of Pheochromocytoma and Paraganglioma. Clinical Chemistry, 60(12), 1486 LP-1499. https://doi.org/10.1373/clinchem.2014.22483299mTc-HYNIC-TOC scintigraphy in a patient with atypical giant paraganglioma in: (a) Anterior and (b) posterior whole-body scintigrams, (c) axial CT scan, (d) axial SPECT/CT fusion. The examination confirmed the expression of somatostatin receptors in peripheral solid areas of the large tumour (arrows). CT, computed tomography. | Eisenhofer, G., & Peitzsch, M. (2014). Laboratory Evaluation of Pheochromocytoma and Paraganglioma. Clinical Chemistry, 60(12), 1486 LP-1499. https://doi.org/10.1373/clinchem.2014.22483218F-FDG PET/CT in SDHB-positive patient; (a) maximum-intensity projection, (b) axial CT slice, (c) fused axial 18F-FDG PET/CT image. The finding reveals the metastatic spread of malignant pheochromocytoma into the liver (yellow arrows) and the left lung (black arrow). 18F-FDG, 18F-fluorodeoxyglucose. | Eisenhofer, G., & Peitzsch, M. (2014). Laboratory Evaluation of Pheochromocytoma and Paraganglioma. Clinical Chemistry, 60(12), 1486 LP-1499. https://doi.org/10.1373/clinchem.2014.224832
Management
Laparoscopic and adrenal sparing surgical intervention following preoperative alpha-blockade is the treatment of choice and usually curative. In malignant pheochromocytomas, radiotherapy and chemotherapy are palliative treatment options
Initial (peripoerative) management:
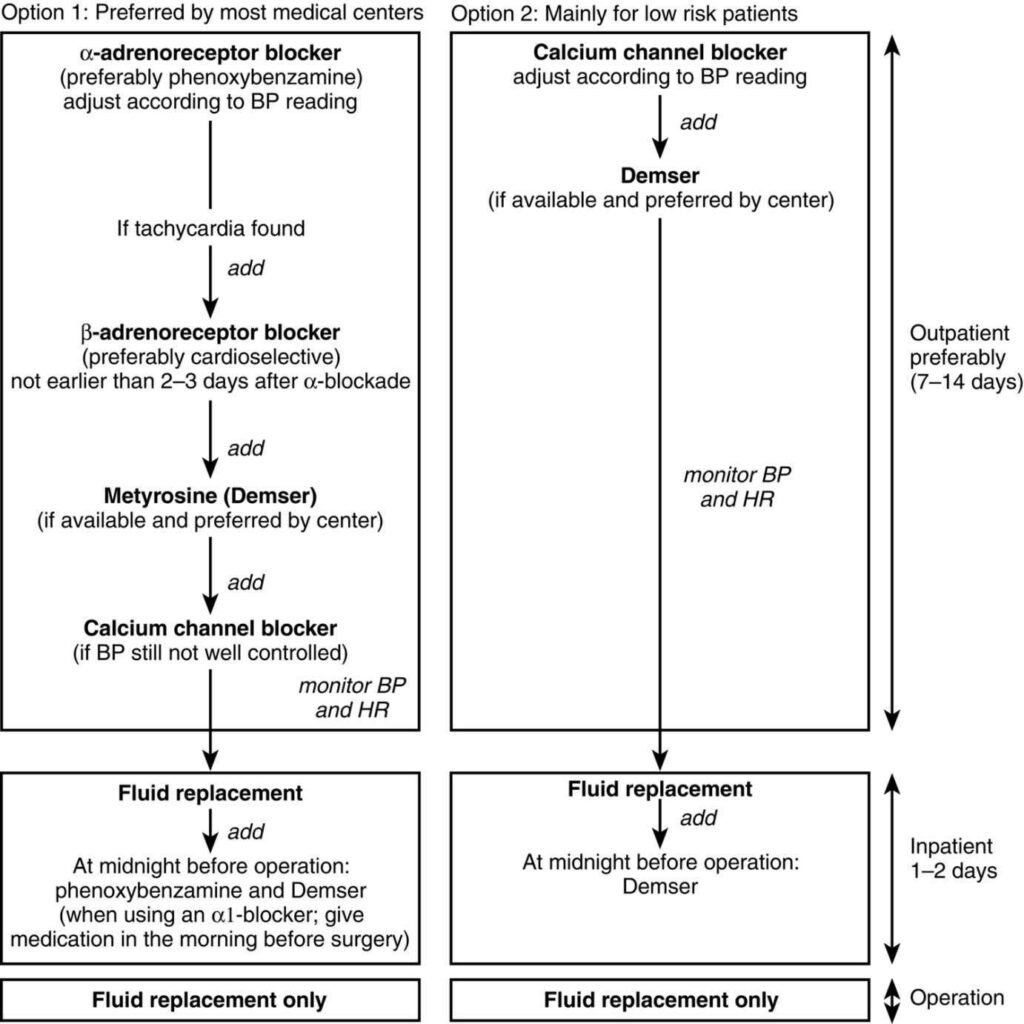
Current recommended preoperative treatment algorithms in patients with pheochromocytoma. Abbreviations: BP = blood pressure; HR = heart rate. | Pacak K: Preoperative management of the pheochromocytoma patient. J Clin Endocrinol Metab 2007;92:4069–4079.
Control hypertension:
Non-selective α-blocker:
Phenoxybenzamine (DOC)
Oral/IV Phentolamine (manage paroxysms)
β-blockers: After alpha blockade
Beta-blockers are not administered until adequate alpha blockade has been established because the stimulation of unopposed alpha-adrenergic receptors can precipitate a hypertensive crisis.
Metyrosine (tyrosine hydroxylase inhibitor)
Malignant PCC:
Nuclear medicine therapy: 131I-MIBG (first-line)
Averbuch’s chemotherapy protocol:
Dacarbazine (600 mg/m2 on days 1 and 2)
Cyclophosphamide (750 mg/m2 on day 1)
Vincristine (1.4 mg/m2 on day 1)
Surgical (definitive) management:
Open resection if tumour > 8-10 cm
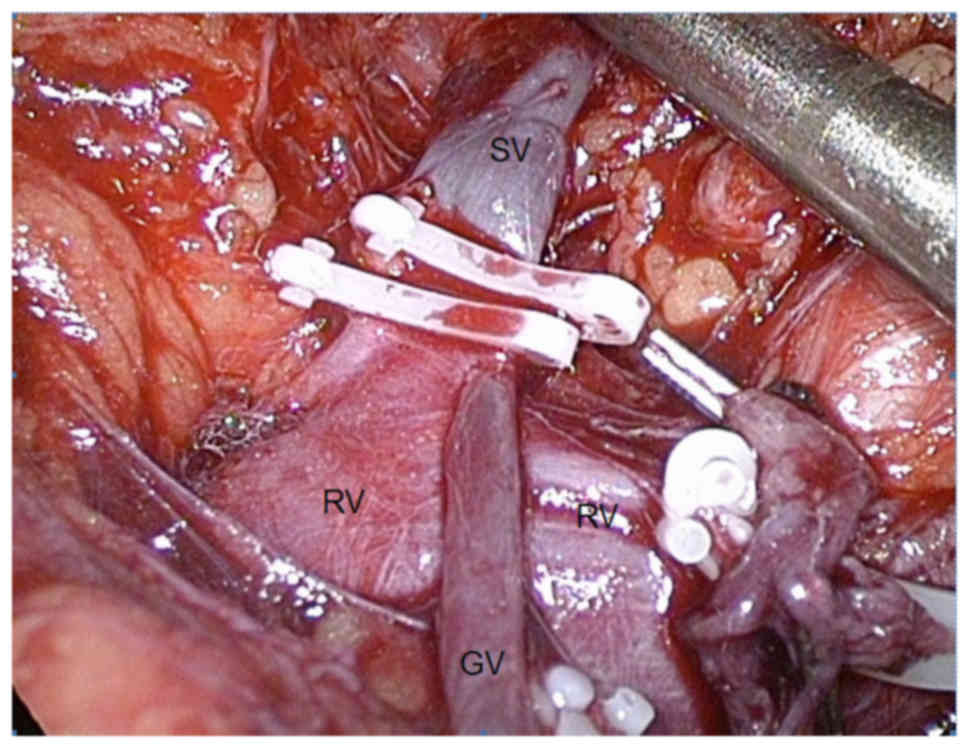
Photograph of a laparoscopic adrenalectomy: exposed left RV and SV, clips placed on the suprarenal vein before attempting further manipulation of the pheochromocytoma. Incidental finding of an anomalous left GV draining into the left suprarenal vein. RV, renal vein; SV, suprarenal vein, GV, gonadal vein. | Eisenhofer, G., & Peitzsch, M. (2014). Laboratory Evaluation of Pheochromocytoma and Paraganglioma. Clinical Chemistry, 60(12), 1486 LP-1499. https://doi.org/10.1373/clinchem.2014.224832